1. INTRODUCTION
Being responsible of 17.9 million deaths each year, and representing 31% of all global deaths, cardiovascular disease (CVD) is the leading cause of mortality worldwide (1). The most common CVDs are stroke and heart attack, accounting for 85% of the deaths (1,2). Regarding the prevention and development of CVD, diet has a crucial role and is considered to be a modifiable risk and preventive factor (3).
Cardiometabolic risk is described as the set of metabolic anomalies, including hypertension, dyslipidemia and dysglycemia, which increase CVD risk in a dose-response manner. Insulin resistance, excess visceral adipose tissue and ectopic fat accumulations are linked to these abnormalities conditioning the components of metabolic syndrome (MetS) (4).
MetS increases the risk of developing CVD by 1.7 (4). This syndrome is defined as a cluster of metabolic abnormalities which include at least three of the following CVD risk factors: high blood pressure, high fasting plasma glucose levels, low HDL cholesterol levels, hypertriglyceridemia and abdominal obesity (4).
On the other hand, ultra-processed foods (UPFs) are products that have been around for decades, but whose production has increased over the years due to new processing technology in the food industry (5). As a result, this increase has also led to the massive worldwide consumption of this type of food, for instance, having a +20,7 % consumption of UPFs in Spain from 1990 to 2010 (4).
However, there is also a growing trend towards eating healthy, organic and sustainable food. Having seen the harmful effects that a diet based on industrial foods can have, people have recently begun to show interest in having a healthier lifestyle (6). In the wake of this massive UPFs consumption, several movements have emerged against them, including Spanish Nutritionist Carlos Ríos’s “Real Fooding” movement. “Real Fooding” is a social movement created around social networks. Its lifestyle consists of eliminating UPFs from the diet and replacing them with real food, hence the name.
The term “ultra-processed food (UPF)” emerged in 2009, which defined the degree of industrial processing and included certain ingredients’ presence or absence in food (4). However, “ultra-processed food” does not have a clear, concise and universal definition. The term has been defined a large number of times, and all differ slightly from each other, but definitions agree that processed food is the transformation of natural or raw products into ingredients or food through one or more physical, chemical or microbiological processes (4). The aim of these transformations is to improve one or more aspects of the product such as its availability, shelf life, appearance, safety or nutritional quality (7).
The NOVA classification developed in Brazil in 2010 is the most widely used system for classifying and estimating the intake of UPFs in epidemiological studies. This system considers the chemical, biological and physical processes to which the food undergoes before consumption, resulting in a total of four food groups (4, 8). This classification will be the one used in this review as well as the one used in the analyzed studies.
The first group in the NOVA classification includes unprocessed or minimally processed foods. That is to say, plant (fruits, seeds, leaves, stems, roots) or animal-derived (offal, eggs, milk, muscle) food presented after harvest, collection or slaughter. This group also includes water, fungi and algae. Minimally processed food refers to food altered so as not to add or introduce any substance, such as removal of inedible or unwanted parts or other processing such as drying, crushing, grinding, fractioning, filtering, roasting, boiling, fermentation, pasteurization, refrigeration or chilling (4, 7, 8).
Second group refers to processed culinary ingredients, which englobes industrial products extracted and purified from food ingredients or other ingredients obtained from nature. This includes ingredients such as oils, butter, sugar and salt as they are extracted either from the first group of food or from nature through pressing, refining, grinding, milling and drying processes. The purpose of such processes is to be combined with foods from group 1 and they are not meant to be consumed by themselves (4, 7, 8).
Third group includes processed foods, in which group 1 foods are modified by the addition of group 2 substances such as oil, sugar, salt or sugar to whole foods in order to increase their durability or to modify their flavor and attractiveness. These are usually additions of two or three ingredients and are known as modified versions of the first category of foods. They are edible on their own or in combination with other foods. Examples of this group are bottled vegetables, canned fish or cheeses (4, 7, 8).
Finally, group 4 refers to UPFs. Prepared mainly or entirely from food-derived substances, this group includes processes such as hydrogenation, hydrolysis; extrusion, molding, reshaping; pretreatment by frying and baking. Sugars, oils, fats and salt are commonly used in this food group, as well as other additives extracted from foods such as casein, lactose, whey and gluten. It also includes hydrogenated or interesterified oils, hydrolyzed proteins, soya protein isolate, maltodextrin, invert sugar and high-fructose corn syrup. Examples of this group are soft drinks, sweets, breaded meats, breakfast cereals, biscuits, fruit juices and fruit nectar drinks, energetic drinks and sweetened yoghurts. This group will be the one studied in this review (4, 7, 8).
Nutrient density (nutrient content in a given volume of food) is lower in highly processed food than in unprocessed or minimally processed foods. Lower nutrient density suggests fewer content of fiber, vitamins, minerals, protective bioactive compounds, trace elements and antioxidants (4, 9). All these compounds contained in food have been shown to be significant multifactorial chronic diseases prevention factors in a number of studies (3). Moreover, UPF has lower satiety and a higher glycemic index, leading to their excessive consumption (10, 11). In addition, consumption of UPF is often linked to a sedentary lifestyle with unhealthy habits such as little exercise, smoking… (7) Therefore, it is not surprising that the consumption of UPFs can be related to a higher risk of chronic diseases such as type 2 diabetes, overweight and obesity; all of which may increase the risk of CVD (12).
However, establishing a clear relationship between consumption of processed foods and health is a greatly complex task (13). This is due to the wide range of foods (with vastly different nutritional profiles) that may be classified in the same NOVA group since it has a very large and generic classification. Furthermore, for a type of processed product (e. g. yoghurt) each company has a different formulation with varying concentrations of ingredients.
Despite NOVA classification being overall a powerful tool, it is also very reductionist and uses a qualitative classification, which makes it difficult to classify foods into the categories when there is limited information available for some given foods. Misclassification may occur if a food frequency questionnaire cannot determine the degree of processing or specific information about a certain food, which may affect the accuracy of studies. This will be taken into consideration when discussing the results.
The aim of this paper is to conduct a systematic review to assess the possible association between the consumption of UPFs and the risk of CVD.
2. SUNJECTS AND METHODS
For the elaboration of this systematic review, the standard informative methods corresponding to the PRISMA (14) statement were followed. Relevant articles were identified by a targeted search of the PubMed scientific database for studies which evaluated the intake of UPF and its effect on the risk of CVD. The search strategy was based on the use of MeSH terms related to ultra-processed food intake (Ultra-processed food OR Fast food) and their effect on the risk of cardiovascular diseases (Cardiovascular disease OR Cardiovascular risk factor). With such terms introduced in the search field, 118 results were obtained. 52 references were excluded after reading the abstract, obtaining 66 articles screened. To narrow down the search, inclusion criteria was applied, based on the following conditions. Articles used had to: a) have free access to the full text; b) be scientific articles published in English or Spanish; c) be studies done in humans; d) be original articles, excluding meta-analysis and reviews.
The titles and/or abstracts of the 36 articles obtained in the final search were reviewed to identify all those that were related to the objective of the study and met the inclusion criteria. A total of 31 studies were excluded due to being studies on diseases other than CVD such as obesity, type 2 diabetes, or not being related to the topic of interest, obtaining a final selection of 5 articles. Subsequently, relevant articles were evaluated in detail to be further included in this article. Furthermore, five additional articles were included from the reference list of the selected studies during the full-text review. Figure 1 shows the flow diagram which, following the PRISMA statement, shows the methodology used for the preparation of this systematic review.

Figure 1. Flow diagram of the selection of articles related to the consumption of UPF and CVD risk
3. RESULTS
All articles included in this review were recently published, issued in the last six years (2015-2021). Regarding the design of the studies, four were prospective cohort studies (15-18), four cross-sectional studies (19-22) and two model studies (23, 24). Out of the 10 studies identified, most of them were carried out in high-income countries. Five were performed in the USA (16-18 ,20-22), one in Spain (21), one in France (15) and one in the UK (23). The two studies left were conducted in Brazil (19,24).
Two studies had a sample size greater than 100,000 subjects (15,16); two studies had a sample size in between 10,000 and 99,999 subjects (17, 20) and the smallest sample size was 56 (19). Participants in two of the identified studies (16, 17) had to be middle aged or elderly subjects (aged 50-71 and 55-74). Study populations in the other studies required subjects that were at least 18 years old, however the average age of the participants was shown to be in the middle-aged range (42.7 (15), 53.5 (18), 62.5 (19)). The studies conducted in Spain and Brazil were cross-sectional studies where subjects were men and postmenopausal women diagnosed with rheumatoid arthritis respectively.
There are certain uniformities in the parameters used in the ten selected studies. The NOVA system classification was used in all studies to define food according to processing, which makes it convenient to group the results obtained and allows to suggest a dose-response relationship. One study (18) included the category «culinary preparations» to food classification for mixed dishes that were demonstrated or thought to be homemade due to lack of detailed information. Despite the homogeneity in the classification of foods according to the degree of processing, the operationalization of the exposure varied among the studied publications. Two different methods for assessing the exposure to UPFs were found in this study: food frequency questionnaires and the 24-hour recall, used in 4 (16-18,21) and 4 (15,19,20,22) studies respectively.
Given that there are other variables that predispose to the development of CVD, this adds another layer of complexity to the challenge of determining the relationship between UPFs and CVD. While it would be interesting to analyze these factors to see if they impact on the UPFs and CVD relation, it is outside the scope of this study due to time constraints.
Table 1 lists the studies that have been used in this review and their main characteristics, classified by type of study.
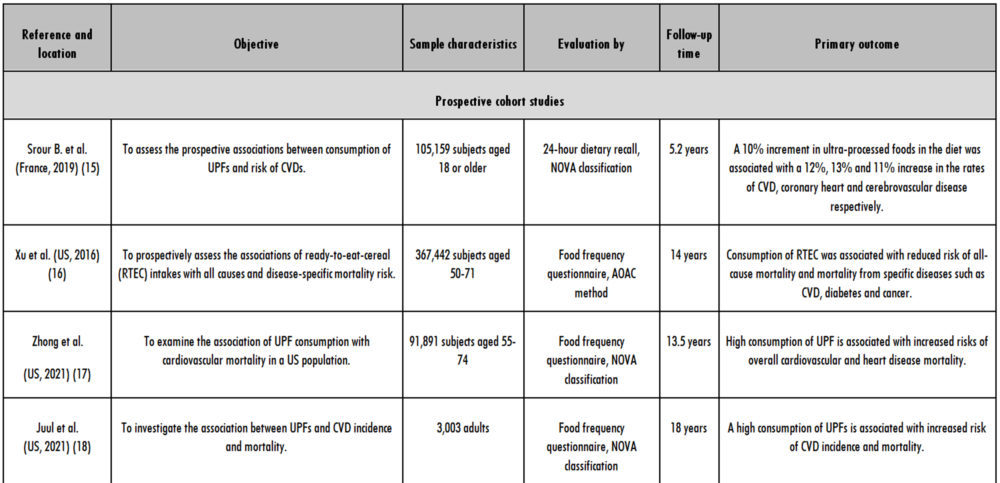
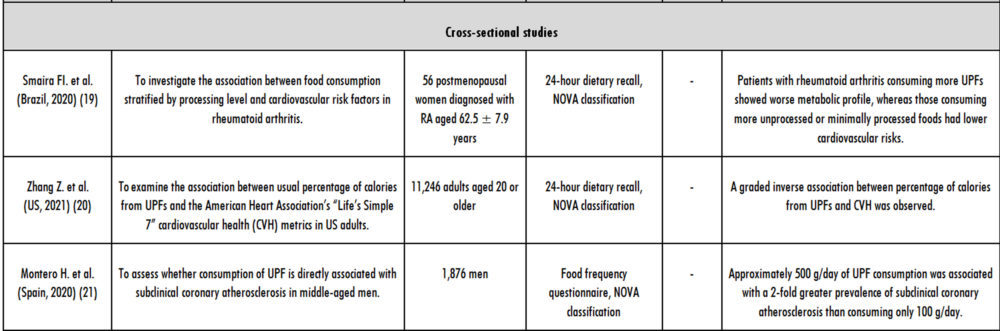
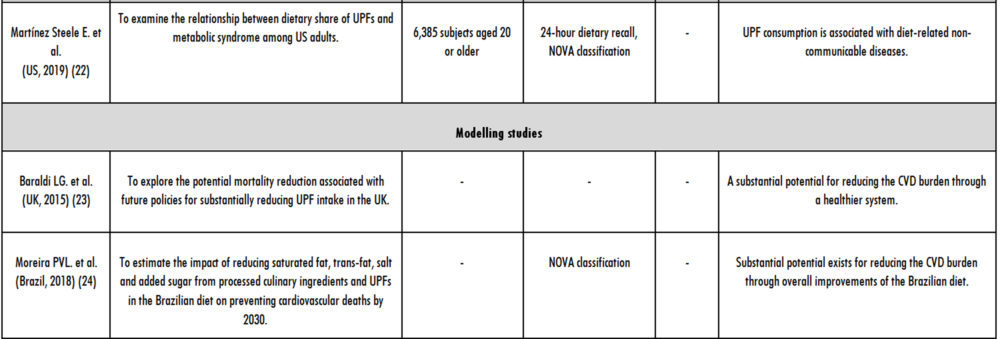
Table 1. Main characteristics of the articles included in this review evaluating the consumption of UPF and CVD risk
4. DISCUSSION
After the review of the scientific literature, it can be affirmed that consumption of UPFs and its relation to cardiovascular risk is a new topic which continues to be investigated. This review identified 10 articles studying the effect that consumption of UPF exerts on CVD. Difference in results may be due to the different study characteristics and factors such as the number of participants, the follow-up time, the country, genetics, lifestyle of participants etc. In order to analyze the topic critically in depth, the obtained results will be studied separately in the following categories: overall CVD, coronary heart disease, cerebrovascular disease, cardiovascular mortality and cluster of diseases (as predisposing factors to the development of CVD).
In the French NutriNet-Santé cohort (15), a 10 % increase in the intake of UPFs was found to significantly increase the incidence of CVD by 12 %. Specifically, a 100g/day increase in consumption of ultra-processed soft drinks was found to be associated with an increased risk of overall CVD. During the follow-up of 518,208 person-years, the total CVD event rates for subjects with high and low UPF consumption was 277 and 242 per 100,000 person-years respectively. This means that in the high intake group 35 additional cardiovascular events occurred every 100,000 person-years. Mathematically speaking, this is equal to an additional event every 2857 person-years. So, to experience a cardiovascular event, 2857 people need to fall into the highest percentile of UPF intake during a one-year follow-up period or one person needs to fall into the highest quarter of UPF intake for 2857 years (25).
This prospective cohort study (15) was carried out at the Sorbonne Paris Cité Epidemiology and Statistics Research Center by 13 authors (with a mean of 216 total studies carried out per author) and has been cited by other 63 articles. With all this, it can be concluded that the study (15) is a reliable source. Juul et al. (2021) (18) found that UPF consumption was associated with higher risk of overall cardiovascular events as well as CVD mortality. Subjects in this study were overweight at baseline, but study has a BMI adjusted model, however, this review takes into consideration that this can have a margin of error. This study established a statistically significant positive association between overall CVD and bread, ultra-processed meat and low-calorie soft drinks in multivariable-adjusted models. However, for sugar-sweetened beverage’s, yoghurts, sweets and desserts, fast foods and other UPFs no statistically significant association with overall CVD was observed. The prospective studies mentioned above (15, 18) have the same motive (consumption of UPFs and incidence of CVD) and were conducted in developed countries (France and USA respectively). A notable difference between the two studies (15,18) is their sample population and the duration of the follow-up. Although the French study (15) has a much higher sample size than US study (18), the latter is by no means small and is carried out by credible authors and is considered reliable. Regarding the duration of follow-up time, Srour et al. (2019) (15) followed up with subjects for 5.2 years, which could be seen as a limitation of this study despite its large sample size. However, Juul et al. (2021) (18) followed up with subjects for 18 years and both studies concluded that consumption of UPFs increases the incidence of CVD.
Moreover, despite having been conducted in developed countries, consumption of UPFs differs from one country to another. Study conducted in France (15) found a 17.6% and 17.3% mean contribution of ultra-processed foods to overall diet in men and women respectively. Although the study (15) itself mentions that their subjects had generally healthier habits than the rest of the French population (less smoking, less likely to be overweight or obese, etc.), it is far from the 58% contribution of ultra-processed foods in the US diet that Juul et al. (2021) (18) obtained. Albeit some differences (country, lifestyle of participants, genetics, intake of ultra-processed foods, etc.), both studies come to the same conclusion which, in our opinion, provides strong evidence that there is a relationship between certain UPFs (i.e., soft-drinks, bread, meat) and CVD incidence because Juul et al.’s (2021) (18) study, with a duration three-times longer, obtained results that corroborate Srour et al.’s (2019) study (15). However, in clinical research, “short-term” and “long-term” definitions are not only very subjective but also highly dependent on pathology, treatment and population. Therefore, an even longer study with a large sample size, of longitudinal design and with similar parameters to the two studies mentioned above should be carried out to try and corroborate these results. Zhang et. al’s (2021) study (20) showed that percentage of calories from UPFs and CVH had a graded inverse association. Study concluded that a higher consumption of UPFs was associated with a lower CVH, obtaining a decrease of 0.14 points in CVH score for every 5% increase in calories from UPF. This US representative study found these results coincide among sex, education, age and poverty-to-income ratio subgroups.
Coronary heart disease is one of the entities included in CVD (26). In the study led by Srour et al. (2019) (15), 109, 116, 125 and 124 per 100,000 person-years coronary heart disease events were obtained for first quartile (low UPF consumers), second quartile, third quartile and fourth quartile (high consumers) respectively. Specifically, coronary heart disease risk was found to be increased by consumption of ultra-processed fats, sauces and meats. Moreover, a second analysis in this study showed a positive association between unprocessed or minimally processed food and lower risk of coronary heart diseases. This study found that if UPFs were increased by 10% in the diet, this would be associated with a statistically significant 13% increase in the incidence of coronary heart disease. Juul et al. (2021) (18) also studied the incidence rates for hard coronary heart disease, obtaining a 2.00 rate per 1,000 person years in participants consuming the least UPFs versus a 4.36 rate per 1,000 person-years in those with the highest intakes, finding a statistically significant association with the intake of bread and salty snack foods in relation to incident hard coronary heart disease. In this study, every additional serving of UPF was associated with a 9% increase in the risk of hard coronary heart disease.
Differences in the foods that are related to coronary heart disease obtained in both studies (15,18) may be due to the composition of UPFs in each country. The main dietary culprit believed to cause coronary heart disease is saturated fat (27). For instance, while composition of main sauces in France has a higher content on saturated fats (butter in bechamel, hollandaise, velouté, etc.), composition of main sauces in US is higher in sugar (ketchup, barbecue sauce, etc.). This could explain why in French study (15) a link is attributed to sauces and coronary heart disease but not in the US (18). Zhong et al. (2021) (17) documented 72.6% heart disease deaths out of a total of 5490 cardiovascular deaths, finding a higher risk of death from heart disease in participants with higher intakes of UPFs than lower consumers. It can be suggested that the relationship between the consumption of UPFs and CVD does exist. However, further studies should be carried out to uncover which foods within this group are the greatest contributors.
Cerebrovascular disease is another of the entities which CVD refers to (26). In the study done by Srour et al. (2019) (15) the total cerebrovascular event rates for subjects with high and low UPF consumption was 163 and 144 per 100,000 person-years respectively, with a statistically significant 11 % increase in the incidence of cerebrovascular disease by raising UPF in the diet by 10%. Salty snacks and sugary products were the foods associated with an increased risk of cerebrovascular disease. However, Zhong et al. (2021) (17) found no significant relationship for cerebrovascular mortality and intake of UPF. This second study documented 5490 cardiovascular deaths, of which 1126 (20.5 %) were cerebrovascular after an average follow-up of 13.5 years. This finding may be because the age of the subjects in the study was 55-74, where other factors and diseases (cancer, COPD, etc.) appear that can cause death, thus displacing death from cerebrovascular disease. Therefore, studies obtained that a high UPF consumption increases the incidence of cerebrovascular disease, but a direct relationship to cerebrovascular mortality has not been established.
Zhong et al. (2021) (17) focused on the relation between cardiovascular mortality and UPF consumption. The results obtained were a positive association between high consumption of UPF and mortality from CVD and heart disease in the US population. According to this study, reducing intake of UPF may help reduce cardiovascular mortality, especially for women. Previous scientific studies have also found that compared with men, women had higher CVD incidence and mortality rates with consumption of soft drinks and processed meats (28, 29). This phenomenon can be explained by the lower concentrations of testosterone that women have than men, since it has been suggested that this hormone plays an important role in CVH maintenance (30) and a negative association between testosterone levels and CVD incidence and death rates have been observed (31-34). In addition, compared with men, women are less compliant with chronic medications. Therefore, these differences between sex may be due to the causes mentioned above and other unknown factors. However, it should not be neglected that these differences may play an important role in cardiovascular mortality and should be investigated in future studies.
Modelling studies also found a positive relation between intake of UPF and cardiovascular mortality. In the UK (23), if the dietary intake of ultra-processed and processed foods is completely replaced with unprocessed or minimally processed foods by 2030, the CVD mortality rate is expected to be reduced by 13 %. A similar approach used in Brazil (24) concluded that if UPFs were reduced by 50 % and replaced with unprocessed or minimally processed foods, with an additional 50% reduction in processed culinary ingredients, CVD mortality would be expected to be reduced by 11 %. However, not all studies yielded a positive relationship between consumption of UPFs and CVD risk. The study conducted by Xu et al. (2016) (16) on ready-to-eat cereals does not establish a positive relation and in fact finds a reducing effect on not only CVD but also in other diseases. Significant inverse associations between intake of ready-to-eat cereal and CVD, type 2 diabetes, cancer and respiratory and infectious diseases and all-cause mortality was found. This may be due to the fiber content of this type of UPF, as it has been shown that consuming high amounts of dietary fiber can significantly reduce CVD morbidity and mortality (35,36). This finding is supported by Juul et al. (2021) (18) whose study found a positive relation between UPF and cardiovascular risk but a decreased risk of overall CVD with the intake of breakfast cereals, having found a statistically significant negative association between breakfast cereals and overall CVD. Therefore, all studies (17, 23, 24), except for one (16), that analyze the relationship between consumption of ultra-processed foods and death from cardiovascular disease observe that by lowering UPFs intake, CVD mortality would decrease. Both prospective studies (16,17) have a large sample size (367, 442 (16) and 91,891 (17)) as well as a long study duration (14 and 13.5 years respectively), and this is strong evidence that their results are reliable.
Thus, in our view, it can be assumed that there is a positive association between the consumption of UPFs and death from CVD, but exceptions exist. For instance, for breakfast cereals which are foods with a high fiber content (can act as a protector against these diseases), not only a positive relationship absent, but the consumption of breakfast cereals can reduce the incidence of cardiovascular disease. Further studies should be conducted to confirm these results and to study whether these exceptions can be applied to other foods in the ultra-processed category.
However, it should be noted that all studies on mortality (16,17,23,24) assume that UPFs and CVD are already somehow related, otherwise studies would be focused on CVD incidence and not mortality. These assumptions may affect the validity of the studies. Zhong et al. (2021) (17) used Srour et al.’s (2019) (15) study to support these assumptions but noted that death from cardiovascular disease due to consumption of ultra-processed foods is still controversial. This may pose a limitation as Srour et al. (2019) (15) concluded that further studies should be carried out to confirm the results obtained in their study. Moreira et al. (2018) (24) justified their assumptions with studies which focused on consumption of added sugar, sodium or fats (compounds which ultra-processed foods have a high content of) and the development of CVD. Likewise, this may pose a weakness since it is assumed that all ultra-processed foods include these compounds. Zhong et al.’s (2021) study (17) is more recent than Moreira et al.’s (2018) study (24), which may be a strength for the first study in terms of availability of literature in this field. However, the paucity of scientific research conducted in this field to date appears to be a limitation for both studies (17, 24).
In regard to cardiovascular risk estimated from intermediate risk factors, the cross-sectional study done on 56 postmenopausal women with rheumatoid arthritis is worth mentioning (19). This study showed that a high consumption of UPFs in these patients was associated with a higher estimated cardiovascular risk and a worse metabolic profile. Conversely, a higher consumption of unprocessed or minimally processed foods was associated with a better cardiovascular risk profile, having a lower 10-year risk of developing CVD.
Montero H. et al.’s (2020) (21) explored the association between subclinical coronary atherosclerosis and high consumption of UPF in middle-aged men. This study found out that people with a high intake of UPF doubled the risk of developing subclinical coronary atherosclerosis. However, subjects in the highest percentile of UPF consumption were more frequently obese, had lower HDL cholesterol levels and performed less physical activity. All these above-mentioned factors predispose to cardiovascular risk events (8,22). Moreover, this study used Coronary Calcium Agatston Score (CACS) as an indicator of calcium deposits. Three categories for CACS were established: 0 for the lowest category (meaning no presence of calcium), > 0 and < 100 for the middle category (presence of calcium), and ≥ 100 for the highest category (moderate to severe subclinical coronary atherosclerosis). Calcium deposits falling into this last category have been demonstrated to increase coronary heart disease. While study found a significant dose-response relation between higher consumption of UPF and risk of progressing from the first and second category to the highest one, no association was found between the risk of progressing from the lowest category to the middle and highest ones and daily consumption of UPF.
Martínez Steele E. et al. (2019) (22) study focused on the relation between UPFs and metabolic syndrome (MetS), which has been demonstrated to increase CVD risk (6). In this study, a higher dietary contribution of UPFs was associated with a higher prevalence of MetS. However, association was not statistically significant if it were not for the adjusted models on age and other potential cofounding factors, which did show significant positive associations. Prevalence of MetS increased by 28 % in the 5th percentile (highest UPF consumption) compared to the 1st percentile (lowest UPF consumption). These findings were particularly strong among young adults, aged between 20 and 39 years and decreased with age. Specifically, the association between the prevalence of MetS and UPF consumption increased by 12 % among people aged 20-39, while for subjects among 40-59, the association’s strength dropped to a third. The explanation the study suggests for this phenomenon is that with increasing age, there may be a decrease in the strength of the association between consumption of UPFs and MetS due to the emergence of other risk factors (obesity, sedentary lifestyle, other aging-related disorders, etc.) that compete with diet as triggers for metabolic syndrome. As to the rationale of all the obtained results, some studies (15, 20, 21) explain that this positive relationship between the consumption of processed foods and the risk of CVD is mainly due to their high content of nutritionally poorer nutrients such as sodium, energy, fats, sugars and their low fiber content, which have already been demonstrated to be high risk factors for cardiometabolic health. Moreover, several studies (15, 20, 21) agreed that an increased risk of CVD in high consumers of UPFs may also partly be due to the displacement of minimally processed foods, resulting in low intake of fruit and vegetables. The low consumption of these foods can affect the results since they are known to be beneficial in preventing CVD (5,6).
Furthermore, the above-mentioned studies (15, 20, 21) refer that another cause of special concern for the obtained results may be the high content on additives on UPFs. High doses of sulphites, monosodium glutamate, emulsifiers (particularly carboxymethylcellulose and polysorbate-80), carrageenan and non-caloric artificial sweeteners were shown to increase the risk of CVD or cardiovascular risk factors such as obesity, metabolic syndrome or insulin resistance (37-40). In addition, Zhang et al. (2021) (20) mentions the high flavoring on UPFs makes these products very palatable, which may result in replacing of the natural satiety mechanisms making people eat more without even being hungry. Lastly, studies allude the association was also due to compounds formed during food processing such as acrylamide as well as contamination by contact materials such as bisphenol A, both of which are associated with an increased risk of CVD (41, 42). Given the paucity of studies, more epidemiological evidence is needed in the future to better understand the relationship between UPFs consumption and CVD risk. Further research needs to be done in order to identify which specific UPFs, compounds and processes have a significant role in the association between UPFs consumption and increased cardiovascular risk. Notably, a recent review addresses potential mechanisms linking ultra-processed foods to CVD risk (43).
5. CONCLUSION
This systematic review provides evidence on the association between the consumption of UPFs and the risk of CVD. After reviewing the literature, it can be concluded that a detailed association between ultra-processed foods and the risk of cardiovascular disease cannot be established due to the multiple variables (NOVA classification, age, sex, country, etc.) that can affect this relationship. As interesting as it may be to study these factors to see if they impact on the UPFs and CVD relation, it is outside the scope of this study due to time constraints.
It can be affirmed that, despite being very reductionist and using a qualitative classification, the NOVA system stands out from other food processing classifications. However, this system presents some limitations. For instance, several studies analyzed in this review supported a negative association between intake of breakfast cereals and increase of CVD, but a positive association between other UPFs (which are classified in the same category as breakfast cereals) and risk of CVD. In addition, there are many factors that influence the nutritional status of the population. The consumption of UPFs is often linked to a sedentary lifestyle in which people, continuously and unwittingly, consume these foods, with little physical activity and unhealthy habits such as smoking (21). Therefore, an increased risk of developing a cardiovascular event cannot be attributed exclusively to the consumption of UPFs. Despite all the limitations stated, we suggest that there is a relationship between consumption of UPFs and CVD. However, further studies should be conducted to raise the level of evidence and corroborate these results, preferably longitudinal design studies.
Ultimately, there is a need to continue generating evidence and to achieve a scientific agreement on this association. Meanwhile, it is essential to promote a diet based on plant-based foods (fruits, vegetables, nuts, legumes, etc.) and to displace foods high in critical nutrients and a high degree of processing. Finally, in order to facilitate access to foods of high nutritional quality and healthy eating patterns further policies should be developed, since there is an increasing evidence of the benefits healthy lifestyle habits have on health conditions and quality of life.
Agradecimientos
Mis primeras palabras son de agradecimiento a los miembros de la Real Academia Nacional de Farmacia por mi elección como académica correspondiente de esta insigne Institución. En particular, al Excmo. Sr. D. Francisco Sánchez-Muniz, académico de número, que impulsó mi candidatura, y me ha apoyado de forma incondicional, haciendo posible la lectura de este discurso.
En mi caso, la incorporación como académico correspondiente de esta Real Academia supone alcanzar un profundo deseo a la vez que un gran honor que agradezco de corazón. Pertenezco por familia a la tercera generación de Farmacéuticos; recuerdo las tardes de verano en Almuñecar, ciudad costera de Granada, cuando apenas llegaba al mostrador, ayudar a ordenar cajas y material en el laboratorio de la botica de mi abuela Amelia. De mi madre Amelia los recuerdos son más vivos. Ella iba a la facultad, tenía prácticas y estudiaba para los exámenes con mi hermano David en el regazo, pintando garabatos; que según decía le ayudaban a memorizar. Acabó la carrera cuando habíamos nacido sus 5 hijos. Enseguida trabajo como farmacéutica comunitaria en Cájar, al pie de Sierra Nevada, a la que se incorporó mi hermano David.
Pero a mí, desde mis estudios en Granada, además de la Farmacia me atraía la idea de ser profesor de Universidad: investigar -me encantaba leer la biografía de Madame Curie-, y dar clase como una manera de ayudar a crecer a gente más joven. Tengo la gran suerte de que mis sueños se han hecho realidad y llevo más de 25 años formando, desde las aulas, a futuros farmacéuticos.
Aparte de estos aspectos de mi biografía, tengo una relación vivencial con esta Ilustre Corporación por su estrecha vinculación con la Facultad de Farmacia de la Universidad de Navarra. Cuando hacía el doctorado pude asistir a las ceremonias -que me quedaron grabadas- de toma de posesión del Prof. Larralde, ex académico de número, q.e.p.d., y años más tarde de la Prof. Fernández Otero como académica correspondiente. Es mi deseo seguir la estela -aunque sea a mucha distancia- de estos y otros “maestros”, muy queridos en nuestra Facultad como el Prof. Monge, también ex académico de número, q.e.p.d. que trabajaron fructífera y generosamente por esta Ilustre Institución.
Reitero mi agradecimiento y admiración a la Real Academia por su rigor científico y buen hacer, en particular a la sección V y a su presidenta la Excma. Sra. Dª Yolanda Barcina, antigua alumna, profesora y fiel amiga de la Universidad de Navarra. A la vez que quiero recordar a la Exma. Sra. Dª Teresa Miras q.e.p.d por su extraordinario trabajo en esta Real Academia, en investigación y en docencia en el campo de la Farmacia. También, a los farmacéuticos comunitarios y de hospital que han estado en primera línea en esta pandemia, particularmente a los que han perdido la vida por cuidar la salud de otros y nos han dejado tan impresionante testimonio de profesionalidad y humanidad. ¡ Qué gran orgullo de compañeras y compañeros, qué grande su espíritu de servicio y compromiso con la sociedad !. Por mi parte en este momento de la historia, tan especial, deseo colaborar en lo que, modestamente, pueda para beneficio de esta noble Institución.
Y ahora permítanme, un breve apunte biográfico: me formé en la Facultad de Farmacia de la Universidad de Granada donde pude disfrutar de las clases magistrales de los Profesores Mataix, Valverde, Sánchez-Medina y Gil. Recién licenciada me trasladé a Pamplona, a la Universidad de Navarra para hacer el doctorado bajo la dirección de la profesora Fernández Otero. En todo momento conté también con el apoyo y cariño del queridísimo D. Jesús, las enseñanzas de ambos y su amor contagioso por la profesión farmacéutica, me ayudaron a encauzar mi trayectoria profesional. Para continuar mi formación, tuve la suerte de formarme en una estancia postdoctoral con la Dra. Henning una mujer con gran prestigio como investigadora y tutora de residentes en el Children Texas Hospital del Baylor College of Medicine (Houston). Y más adelante aprendí técnicas de biología molecular con el Dr. Avruch en el Massachusetts General Hospital de Harvard Medical School en Boston. En 2001, ya como profesora, fui invitada por el Servicio Alemán de Intercambio Académico, al laboratorio del Dr. Hebebrand para investigar en genética de la obesidad. El profesor, un alemán generoso y abierto, me ofreció su casa para que cocinara paella e hiciéramos fiesta española para todo el departamento.
Sin todos y cada uno de esos encuentros, es imposible entender mi presente en el ámbito profesional. Pero más que ninguno sin mi familia, mis colegas y mis amigas y amigos, que a lo largo de mi trayectoria vital, han estado siempre cercanos, asequibles. A Dios y a ellos les debo mucho más que un caluroso agradecimiento.
Aprovecho esta tribuna también para hacer llegar mi más cálido y afectuoso agradecimiento a la Universidad de Navarra -que propició mi enriquecimiento humano y profesional y que facilita mi permanente deseo de servicio a los estudiantes y a la sociedad-, a mis mentores, a mis compañeros de trabajo en la Facultad, a cada profesor, alumno y empleado. Particularmente, a cada una de las jóvenes doctoras con las que tanto he compartido y disfrutado. Me gustaría nombrarlos a todos, pero pienso que no debo agotar la paciencia del auditorio.
En el plano personal, a mis padres y hermanos, particularmente a mi padre que trabajó en esta villa más de 20 años, con gran dedicación y acierto, al servicio de la justicia, desde su querido Palacio de las Salesas; me conmueve recordar su cariño, su “hacer el bien” y su espléndida coherencia cristiana de vida.
Naturalmente, quiero recordar también a mis “maestros y compañeros de camino”, de los que aprendí a soñar, de su talante generoso y magnánimo en el que se aúnan los grandes ideales con el cuidado y la atención al quehacer pequeño y a veces gris de cada día. A Dios y a todos, ellas y ellos, debo, con la más absoluta certeza, el camino recorrido que me ha conducido hasta aquí.
6. REFERENCIAS
- Cardiovascular diseases (CVDs) [Internet]. Who.int. [cited 2021 Apr 10]. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation [Internet]. 2015;131(4):e29-322.
- Fardet A, Chardigny J-M. Plant-based foods as a source of lipotropes for human nutrition: a survey of in vivo studies. Crit Rev Food Sci Nutr. 2013;53(6):535–90.
- Babio N, Casas-Agustench P, Salas-Salvadó J. ALIMENTOS ULTRAPROCESADOS: Revisión crítica, limitaciones del concepto y posible uso en salud pública [Internet]. nutricio.urv.cat. 2021 [cited 2021 Jan 6].
- Marti A. Ultra-processed foods are not “real food” but really affect your health. Nutrients. 2019;11(8):1902.
- Ramachandran D, Kite J, Vassallo AJ, Chau JY, Partridge S, Freeman B, et al. Food trends and popular nutrition advice online – implications for public health. Online J Public Health Inform. 2018;10(2):e213.
- Martí del Moral A, Calvo C, Martínez A. Ultra-processed food consumption and obesity-a systematic review. Nutr Hosp. 2021;38(1):177–85.
- Monteiro CA, Cannon G, Moubarac J-C, Levy RB, Louzada MLC, Jaime PC. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutrition. Cambridge University Press; 2018;21(1):5–17.
- Moubarac J-C, Batal M, Louzada ML, Martinez Steele E, Monteiro CA. Consumption of ultra-processed foods predicts diet quality in Canada. Appetite. 2017;108:512–20.
- Fardet A, Méjean C, Labouré H, Andreeva VA, Feron G. The degree of processing of foods which are most widely consumed by the French elderly population is associated with satiety and glycemic potentials and nutrient profiles. Food Funct. 2017;8(2):651–8.
- Fardet A. Minimally processed foods are more satiating and less hyperglycemic than ultra-processed foods: a preliminary study with 98 ready-to-eat foods. Food Funct. 2016;7(5):2338–46.
- Fardet A, Boirie Y. Associations between diet-related diseases and impaired physiological mechanisms: a holistic approach based on meta-analyses to identify targets for preventive nutrition. Nutr Rev. 2013;71(10):643–56.
- Alonso-Pedrero L, Ojeda-Rodríguez A, Martínez-González MA, Zalba G, Bes-Rastrollo M, Marti A. Ultra-processed food consumption and the risk of short telomeres in an elderly population of the Seguimiento Universidad de Navarra (SUN) Project. Am J Clin Nutr. 2020;111(6):1259–66.
- Urrútia G, Bonfill X. Declaración PRISMA: una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis. Med Clin (Barc). 2010;135(11):507–11.
- Srour B, Fezeu LK, Kesse-Guyot E, Allès B, Méjean C, Andrianasolo RM, et al. Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé). BMJ. 2019;365:l1451.
- Xu M, Huang T, Lee AW, Qi L, Cho S. Ready-to-eat cereal consumption with total and cause-specific mortality: Prospective analysis of 367,442 individuals. J Am Coll Nutr. 2016;35(3):217–23.
- Zhong G-C, Gu H-T, Peng Y, Wang K, Wu Y-Q-L, Hu T-Y, et al. Association of ultra-processed food consumption with cardiovascular mortality in the US population: long-term results from a large prospective multicenter study. Int J Behav Nutr Phys Act. 2021;18(1):21.
- Zhang Z, Jackson SL, Martinez E, Gillespie C, Yang Q. Association between ultraprocessed food intake and cardiovascular health in US adults: a cross-sectional analysis of the NHANES 2011-2016. Am J Clin Nutr. 2021;113(2):428–36.
- Smaira FI, Mazzolani BC, Peçanha T, Dos Santos KM, Rezende DAN, Araujo ME, et al. Ultra-processed food consumption associates with higher cardiovascular risk in rheumatoid arthritis. Clin Rheumatol. 2020;39(5):1423–8.
- Juul F, Vaidean G, Lin Y, Deierlein AL, Parekh N. Ultra-processed foods and incident cardiovascular disease in the Framingham offspring study. J Am Coll Cardiol. 2021;77(12):1520–31.
- Montero-Salazar H, Donat-Vargas C, Moreno-Franco B, Sandoval-Insausti H, Civeira F, Laclaustra M, et al. High consumption of ultra-processed food may double the risk of subclinical coronary atherosclerosis: the Aragon Workers’ Health Study (AWHS). BMC Med. 2020;18(1):235.
- Martínez Steele E, Juul F, Neri D, Rauber F, Monteiro CA. Dietary share of ultra-processed foods and metabolic syndrome in the US adult population. Prev Med. 2019;125:40–8.
- Baraldi LG, Moreira PVL, Moubarac J-C, Monteiro CA, Newton A, Capewell S, et al. Comparing different policy scenarios to reduce the consumption of ultra-processed foods in UK: Impact on cardiovascular disease mortality using a modelling approach. PLoS One. 2015;10(2):e0118353.
- Moreira PVL, Hyseni L, Moubarac J-C, Martins APB, Baraldi LG, Capewell S, et al. Effects of reducing processed culinary ingredients and ultra-processed foods in the Brazilian diet: a cardiovascular modelling study. Public Health Nutr. 2018;21(1):181–8.
- Andrade C. Ultraprocessed food and cardiovascular risk: Estimating the Number Needed to Harm in an unfamiliar situation. Indian J Psychol Med. 2019;41(5):501–2.
- Olvera Lopez E, Ballard BD, Jan A. Cardiovascular Disease. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
- DiNicolantonio JJ, OKeefe JH. Added sugars drive coronary heart disease via insulin resistance and hyperinsulinaemia: a new paradigm. Open Heart. 2017;4(2):e000729.
- Eshak ES, Iso H, Kokubo Y, Saito I, Yamagishi K, Inoue M, et al. Soft drink intake in relation to incident ischemic heart disease, stroke, and stroke subtypes in Japanese men and women: the Japan Public Health Centre-based study cohort I. Am J Clin Nutr. 2012;96(6):1390–7.
- Wang X, Lin X, Ouyang YY, Liu J, Zhao G, Pan A, et al. Red and processed meat consumption and mortality: dose-response meta-analysis of prospective cohort studies. Public Health Nutr. 2016;19(5):893–905.
- Cruz-Topete D, Dominic P, Stokes KY. Uncovering sex-specific mechanisms of action of testosterone and redox balance. Redox Biol. 2020;31(101490):101490.
- Corona G, Rastrelli G, Di Pasquale G, Sforza A, Mannucci E, Maggi M. Endogenous Testosterone Levels and Cardiovascular Risk: Meta-analysis of Observational Studies. J Sex Med. 2018;15(9):1260–71.
- Khaw K-T, Dowsett M, Folkerd E, Bingham S, Wareham N, Luben R, et al. Endogenous testosterone and mortality due to all causes, cardiovascular disease, and cancer in men: European prospective investigation into cancer in Norfolk (EPIC-Norfolk) Prospective Population Study. Circulation. 2007;116(23):2694–701.
- M Webb C, Collins P. Role of testosterone in the treatment of cardiovascular disease. Eur Cardiol. 2017;12(2):83–7.
- Ohlsson C, Barrett-Connor E, Bhasin S, Orwoll E, Labrie F, Karlsson MK, et al. High serum testosterone is associated with reduced risk of cardiovascular events in elderly men. The MrOS (Osteoporotic Fractures in Men) study in Sweden. J Am Coll Cardiol. 2011;58(16):1674–81.
- McRae MP. Dietary fiber is beneficial for the prevention of cardiovascular disease: An umbrella review of meta-analyses. J Chiropr Med. 2017;16(4):289–99.
- Barber TM, Kabisch S, Pfeiffer AFH, Weickert MO. The health benefits of dietary fibre. Nutrients. 2020;12(10):3209.
- Zhang Q, Bai Y, Yang Z, Tian J, Meng Z. The molecular mechanisms of sodium metabisulfite on the expression of K ATP and L-Ca2+ channels in rat hearts. Regul Toxicol Pharmacol. 2015;72(3):440–6.
- Singh K, Ahluwalia P. Effect of monosodium glutamate on lipid peroxidation and certain antioxidant enzymes in cardiac tissue of alcoholic adult male mice. J Cardiovasc Dis Res. 2012;3(1):12–8.
- Chassaing B, Koren O, Goodrich JK, Poole AC, Srinivasan S, Ley RE, et al. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature. 2015;519(7541):92–6.
- Bhattacharyya S, O-Sullivan I, Katyal S, Unterman T, Tobacman JK. Exposure to the common food additive carrageenan leads to glucose intolerance, insulin resistance and inhibition of insulin signalling in HepG2 cells and C57BL/6J mice. Diabetologia. 2012;55(1):194–203.
- DeJarnett N, Conklin DJ, Riggs DW, Myers JA, O’Toole TE, Hamzeh I, et al. Acrolein exposure is associated with increased cardiovascular disease risk. J Am Heart Assoc. 2014;3(4).
- Rancière F, Lyons JG, Loh VHY, Botton J, Galloway T, Wang T, et al. Bisphenol A and the risk of cardiometabolic disorders: a systematic review with meta-analysis of the epidemiological evidence. Env Environ Health. 2015;14(1):46.
- Juul F, Vaidean G, Parekh N. Ultra-processed Foods and Cardiovascular Diseases: Potential Mechanisms of Action. Adv Nutr 2021 May 3; Online ahead of print.
