1. Introduction
EULAR provides extensive and continually updated recommendations for the management of various rheumatological diseases (1). These guidelines generally recommend initiating treatment with a biologic disease-modifying antirheumatic drug (bDMARD) or a targeted synthetic disease-modifying antirheumatic drug (tsDMARD) when the desired target is not achieved with prior therapies. However, they do not specify which drug should be chosen as the initial option. Drug selection is based on a trial-and-error approach, considering patient characteristics, drug availability, established cost-efficiency protocols, and the experience of the treatment center. The Rheumatology Service (RS) at a tertiary hospital in northwest Spain conducts weekly multidisciplinary meetings to determine the most appropriate bDMARD or tsDMARD for each patient. These sessions are attended by the entire RS team, including physicians, nurses, clinical researchers, and the pharmacist responsible for the rheumatology area. Additionally, specialists from other fields, such as gastroenterology, dermatology, and pulmonology, are invited as needed. Before each session, patient data is sent by email for review.
During each meeting, the physician responsible for a given patient presents the case, detailing the medical history, comorbidities, previous treatments, current disease status, and the proposed treatment. This presentation is followed by a group discussion, leading to a consensus on the clinical approach or therapeutic management strategy.
Each rheumatologist maintains a general clinical consultation with their patients. When a patient is identified as a candidate for initiating bDMARD or tsDMARD therapy or for switching treatments due to inadequate response or safety concerns, the case is presented during these weekly sessions. Patients considered eligible for treatment are followed in dedicated clinical consultations at 3 and 6 months after therapy initiation. If their condition remains stable during this period, they are returned to routine consultations with their treating rheumatologist (see Figure 1).
This descriptive study aims to present our experience with these sessions, evaluate the concordance between the treatment selected in the session and that ultimately initiated, and assess the treatment efficacy at 3 and 6 months post-initiation in a real-world setting.
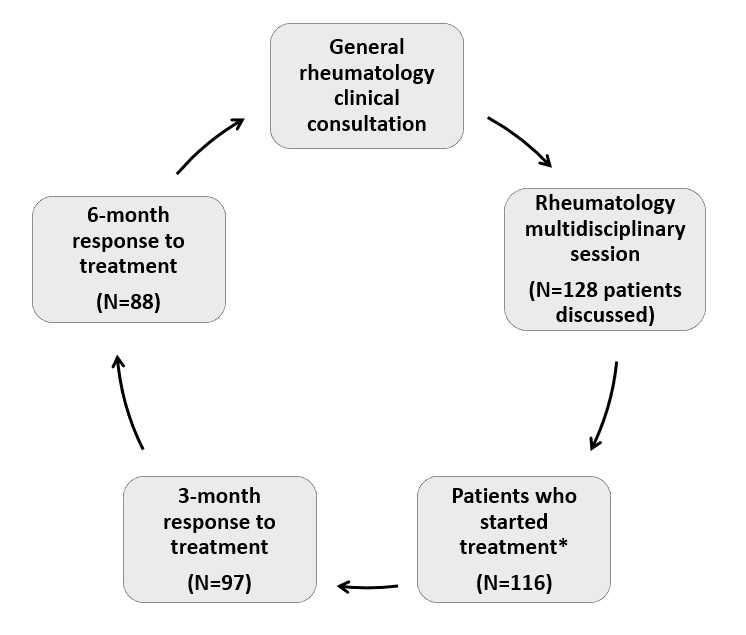
Figure 1. Patient flow across different rheumatology healthcare consultations, summarizing the study findings. *Treatment refers to a biological or targeted synthetic disease-modifying antirheumatic drug.
2. Methods
This retrospective descriptive study included all patients discussed in these sessions between September 2023 and March 2024. Data collected from electronic medical records included baseline characteristics (sex, age), clinical features (diagnosis), session and treatment initiation dates, concordance between the proposed and initiated treatment, treatment continuation, and response at 3 and 6 months. The follow-up period spanned from September 2023 to October 2024, ensuring that all patients completed six months of treatment.
Treatment response was recorded as a dichotomous variable (yes/no) and assessed using two criteria: clinical judgment and specific scales tailored to each condition. Depending on data availability, the scales used included DAS28 or DAS28-CRP for rheumatoid arthritis (RA) and juvenile idiopathic arthritis (JIA), SLEDAI for systemic lupus erythematosus (SLE), ASDAS-CRP, DAS28, DAS28-CRP or BASDAI for spondyloarthritis (SpA), and psoriatic arthritis (PsA). For conditions such as giant cell arteritis (GCA), uveitis, Sjögren’s syndrome (SS), vasculitis, Behcet’s disease, IgG4-related disease, scleritis, and granulomatous disease, response was assessed solely by clinical judgment.
Qualitative variables were described as frequency (n) and percentage, while quantitative variables were presented as mean ± standard deviation.
This study received approval from the Clinical Research Ethics Committee of Galicia and was conducted in accordance with the Helsinki Declaration of Good Clinical Practices.
3. Results
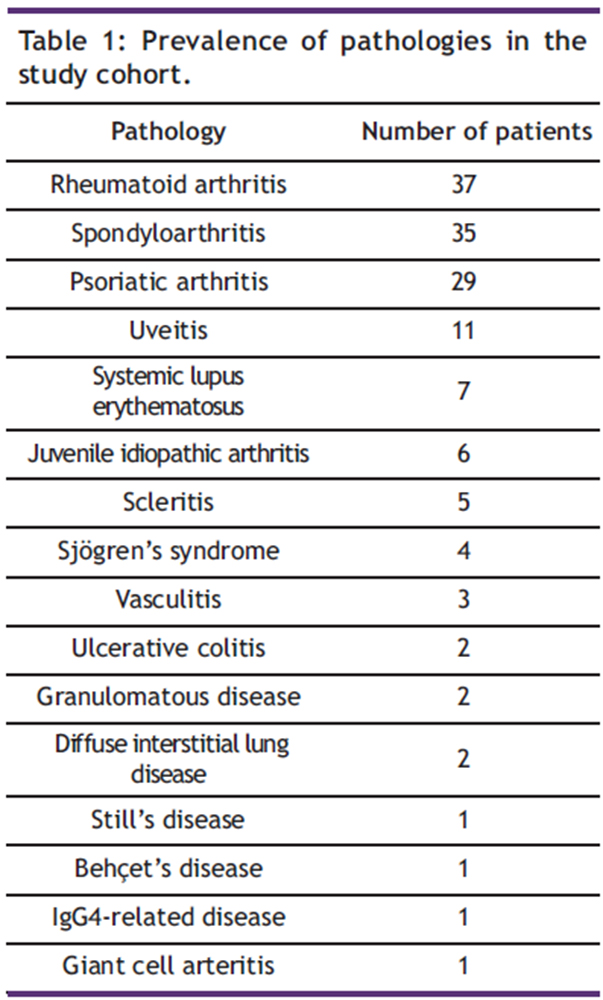
During the study period, 128 patients were discussed, of whom 94 were women (73%) and 34 were men (27%), with a mean age of 47.3±15.5 years. The distribution of diseases in the cohort is presented in Table 1. The most prevalent were RA (n=37), SpA (n=35), and PsA (n=29). A single patient could be diagnosed with more than one condition.
Table 1: Prevalence of pathologies in the study cohort.
In 92% of cases (n=118), there was agreement between the therapeutic approach decided in the session and that ultimately implemented. Discrepancies occurred in 8% of cases (n=10), including three patients who started a different drug than proposed, two who enrolled in a clinical trial, two who voluntarily declined treatment, and two in which treatment was not initiated. In one additional case, the patient continued with their existing treatment.
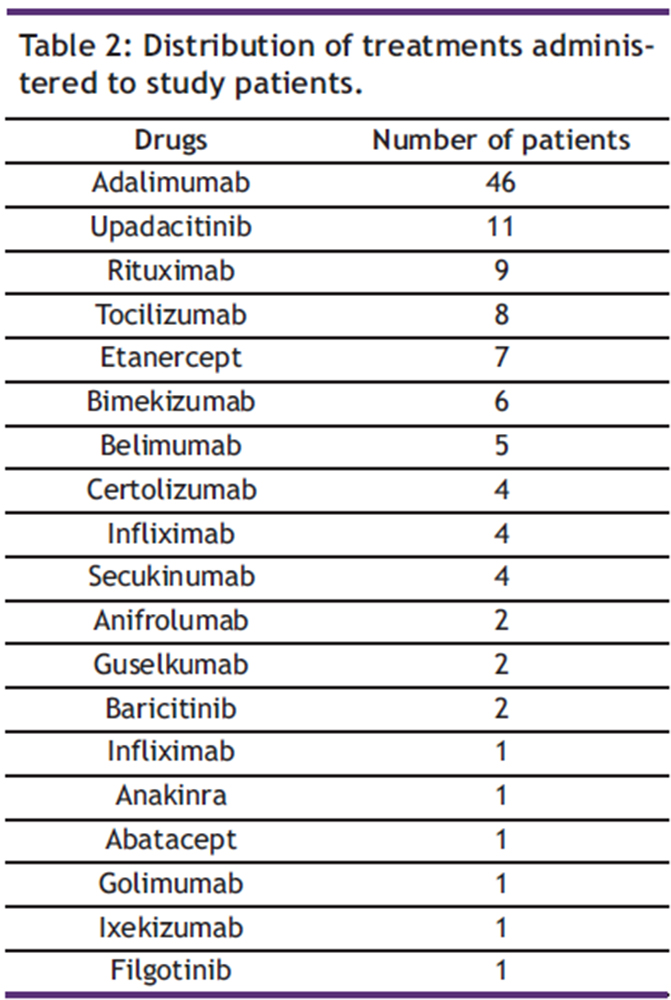
Of the 128 patients, 116 initiated treatments with a bDMARD (n=102) or tsDMARD (n=14). The treatments administered are detailed in Table 2. The average time from the session to treatment initiation was 24±16.2 days. In 14 patients, treatment was delayed by more than 40 days, mainly due to tuberculosis chemoprophylaxis, administration of live vaccines, or hospitalization.
Table 2: Distribution of treatments administered to study patients.
Before reaching 3 months, 19 patients discontinued treatment due to inefficacy (n=9), safety (n=6), or other reasons (n=4). At 3 months, 97 of 116 patients (84%) continued with the same drug. Before reaching 6 months, an additional 9 patients discontinued treatment due to inefficacy (n=5), safety (n=2), or other reasons (n=2). At 6 months, 88 of 116 patients (76%) remained on the same bDMARD or tsDMARD (see Figure 2).
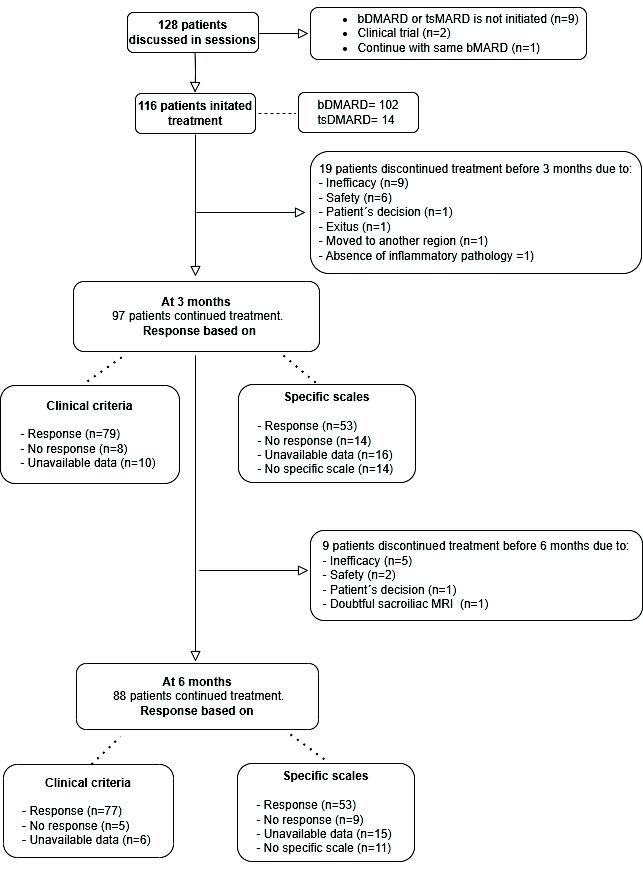
Figure 2. Flowchart of study patients during follow-up.
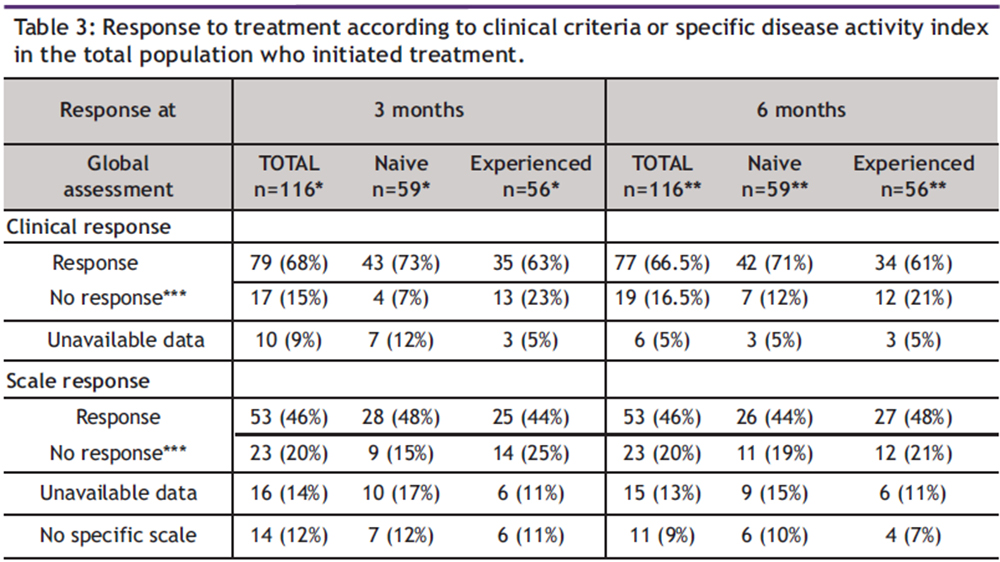
Based on clinical criteria, 68% of patients showed a positive response to treatment at 3 months, and 15% did not respond. Similarly, 66% responded at 6 months, and 16% did not. However, using specific response scales, 46% of patients responded at 3 months, and 20% did not. Additionally, 12% did not have a particular scale recorded. Also at 6 months, 46% responded and 20% did not. No particular scale in 9%. Better response rates were observed among treatment-naïve patients (Table 3).
Table 3: Response to treatment according to clinical criteria or specific disease activity index in the total population who initiated treatment.
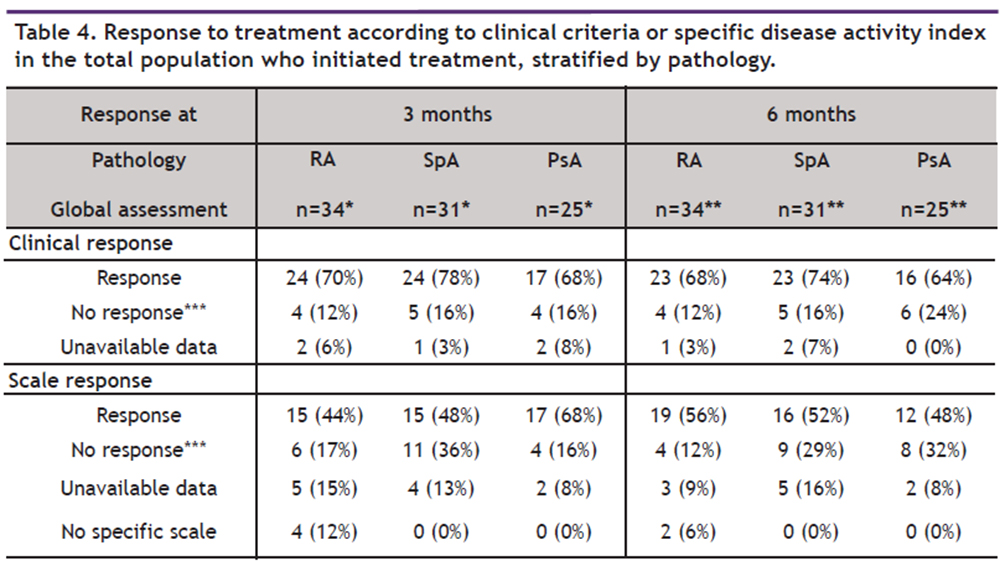
Given that RA, SpA, and PsA were the predominant conditions, a stratified analysis was performed for these patients (Table 4).
Table 4. Response to treatment according to clinical criteria or specific disease activity index in the total population who initiated treatment, stratified by pathology.
4. Discussion
To our knowledge, this is the first real-world study describing the experience of a multidisciplinary team in selecting initial bDMARD or tsDMARD for rheumatologic conditions. We have not identified any studies that specifically examine this type of meeting within healthcare services for decision-making and task execution. In our study, we observed high concordance in therapeutic decisions and notably high drug retention rates by the end of the study. However, the efficacy response varied depending on the evaluation criteria used.
Gukova et al. conducted a study in which they developed an interdisciplinary care pathway for early RA. It consisted of a four-phase approach to improve triage, diagnosis, and management. They concluded that an interdisciplinary approach is essential to deliver the highest quality care to these patients (2). In our study, 128 patients were discussed during the weekly sessions, with a 92% concordance rate between session decisions and implemented therapy.
Of the 116 patients who initiated therapy, 76% remained on the same drug at 6 months. Previous studies reported comparable 6-month drug retention rates to those observed in our study, ranging from 75% to 88% (3-6).
Comparing our data with previous studies is challenging due to the variability in how response is defined and measured. While some studies report remission rates, others focus on low disease activity (LDA) or use the EULAR response criteria. Our descriptive study assessed response rates (yes/no) based on clinical judgment and specific assessment scales. Furthermore, our cohort included a heterogeneous mix of rheumatic diseases and both treatment-naïve and experienced patients, reflecting the diverse clinical scenarios encountered in routine practice. The primary aim of this study was to describe our experience with shared decision-making in collaboration with patients and within the multidisciplinary team.
In the study by Ørnbjerg et al. involving patients with SpA treated with their first anti-TNF, the 6-month response rates were as follows: ASDAS inactive disease/BASDAI < 40 rates were 33%/72% (LUNDEX-adjusted: 27%/59%), and ASAS 20/40 response rates were 64%/49% (LUNDEX-adjusted 52%/40%) (6). Fewer response rates were reported in the study by Mease et al., where 20% and 14% of patients with ankylosing spondylitis initiating bDMARD achieved ASAS20 and ASAS40, respectively, at 6 months. Additionally, only 34% achieved an optimal treatment response (ASDAS, <2.1). Better responses were observed in treatment-naïve patients compared to experienced ones (7).
Brahe et al. examined PsA patients and found 6-month remission rates based on DAS28/DAPSA were 56%/27% (LUNDEX-adjusted: 45%/22%). The ACR20/50/70 response rates at 6 months were 53%, 38%, and 22%, respectively (4). In the study by Colombo et al. evaluating the effectiveness of biologics in PsA, 6-month response rates using EULAR DAS28 criteria were 71.8%, while ACR20/50/70 responses were 41.2%, 29.4%, and 17.1%, respectively (8).
For RA, Alten et al. reported that 6-month remission rates were 25.6% and 18.5% for patients treated with baricitinib and those treated with other tsDMARDs or bDMARDs, respectively. The corresponding proportions of patients achieving LDA were 36.8% and 37.3%, respectively (5). In the study by Santos et al., 46.4% of RA-experienced patients treated with a bDMARD achieved remission or LDA according to CDAI at 6 months; however, LUNDEX adjustments showed lower response rates (3). Ramirez et al. showed in their study that at 6 months, 75.6% of RA patients treated with JAK inhibitors achieved remission and LDA, while 63.6% of patients with SpA achieved remission/LDA, and 87.5% of patients with PsA achieved low activity (9).
As outlined above, response rates across studies vary depending on the underlying pathology and whether the patients were treatment-naïve or experienced with b/tsDMARDs. Notably, all studies assessed responses using validated indices or scales tailored to the specific condition.
In our study, the overall scale-based response rate at 6 months was 46%. When stratified by pathology, higher response rates were observed: 56% in RA, 52% in SpA, and 48% in PsA. Furthermore, response rates were higher when assessed using clinical response criteria. The overall clinical response rate was 66%, with similar rates observed in RA (68%) and PsA (64%), and a higher rate in SpA (74%).
A notable difference in our study emerges when comparing overall 6-month positive response rates based on clinical criteria (66%) versus specific assessment scales (46%). This disparity can be partly attributed to the absence of specific scales for certain pathologies, making scale-based assessments inapplicable in approximately 10% of cases, as well as the unavailability of data for 13% of the patients. Approximately half of the missing data regarding uncalculated scales or missed follow-up visits at 3 or 6 months pertain to patients from clinical trials or other healthcare areas. Another contributing factor could be that patients often rated their disease more negatively compared to their physicians did.
From our perspective, the clinician’s evaluation holds greater significance than scale-based assessments alone, particularly when the latter are feasible but influenced by various factors. These include infectious processes, the patient’s emotional state, and other conditions that affect acute-phase reactants. Additionally, mechanical pain or comorbidities such as fibromyalgia can further distort scale results (10). Clinicians take these complex factors into account when determining treatment response.
This study highlights some limitations and areas for improvement in our clinical practice. First, its purely descriptive nature precludes causal inference or comparisons between groups. Second, some data points were unavailable for response evaluation, either because visits were not conducted within the specified timeframe or the corresponding scales were not completed. This may also occur when patients do not attend follow-up appointments or fail to complete the necessary laboratory tests. Third, as this study relies on real-world data, it is evident that the clinical workload sometimes does not permit complete data collection. While the number of patients with missing data for response calculation is not high, there is always potential for improvement. Finally, the absence of the DAPSA scale in evaluating treatment response for PsA represents another limitation. Although increasingly recommended in recent years, it was not part of our evaluation protocols at the time. Moving forward, we plan to incorporate the DAPSA scale into our assessments to enhance the precision of our evaluations.
5. Conclusions
These multidisciplinary meetings provide a framework for collaborative therapeutic decision-making and may support the selection of the most appropriate treatment for each patient. They also offer opportunities for communication among the various healthcare professionals involved. Although this study did not directly measure improvements in decision-making or communication, the descriptive results suggest that such meetings could be a valuable approach and potentially implementable in other hospitals. Our efficacy findings are consistent with the response rates described in the literature. Nonetheless, there is room for improvement in data collection and in-patient response rates. By sharing these real-world observations, we aim to inform the broader professional community and contribute to ongoing efforts to optimize the management of patients with rheumatic diseases.
Acknowledgement: We would like to thank the entire Rheumatology and Pharmacy departments for their collaboration, as well as all the patients for their invaluable support.
Funding: This study has been funded by Instituto de Salud Carlos III (ISCIII) through the projects
PMP15/00032, and PMP22/00101 co-funded by the European Regional Development Fund ‘A way to make Europe’; funded by ISCIII, co-funded by the European Union and project PI23/00818. SR-S was supported by ISCIII Programa Rio Hortega CM22/00210. LG is a PhD student supported by Cátedra FSR-UDC, Universidad de A Coruña.
Conflict of interest: Dr. Francisco Blanco has received grants or contracts from speaker fees from Abbvie, Bristol Myers Squibb, Roche, Servieer, Novartis, Horizon Therapeutics Ireland DAC, ITF RESEARCH PHARMA S.L.U., GSK Research, Pfizer, Sanofi-Aventis, Grunenthal, Lilly, Merck Healthcare, KgaA, LG Chem, Ltd, UCB, Janssen, Amgen, Regeeron, Alkem Labortories Ltd, Grunenthal, Sun Pharma Global FZE, Kiniksa Pharmaceuticals, GmbH, speakers fees from Medicamenta-Ecuador, Grunenthal and Asofarma, support attending meetings from UCB, Abbie and Celgen. All of them unrelated to the study presented in this manuscript.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process: During the preparation of this work, the authors used ChatGPT and Grammarly to improve readability and language. After using these tools, the authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
6. References
- EULAR [Internet]. [citado 28 de noviembre de 2024]. Recommendations Management. Available at: https://www.eular.org/recommendations-management
- Gukova X, Hazlewood GS, Arbillaga H et al. Development of an interdisciplinary early rheumatoid arthritis care pathway. BMC Rheumatol. 2022;6(1):35.
- Santos-Faria D, Tavares-Costa J, Eusébio M, et al. Tocilizumab and rituximab have similar effectiveness and are both superior to a second tumour necrosis factor inhibitor in rheumatoid arthritis patients who discontinued a first TNF inhibitor. Acta Reumatol Port. 2019;44(2):103-13.
- Brahe CH, Ørnbjerg LM, Jacobsson L, et al. Retention and response rates in 14 261 PsA patients starting TNF inhibitor treatment—results from 12 countries in EuroSpA. Rheumatology (Oxford). 2020;59(7):1640-50.
- Alten R, Burmester GR, Matucci-Cerinic M, et al. The RA-BE-REAL Multinational, Prospective, Observational Study in Patients with Rheumatoid Arthritis Receiving Baricitinib, Targeted Synthetic, or Biologic Disease-Modifying Therapies: a 6-Month Interim Analysis. Rheumatol Ther. 2023;10(1):73-93.
- Ørnbjerg LM, Brahe CH, Askling J, et al. Treatment response and drug retention rates in 24,195 biologic-naïve patients with axial spondyloarthritis initiating TNFi treatment: routine care data from 12 registries in the EuroSpA collaboration. Ann Rheum Dis. 2019;78(11):1536-44.
- Mease PJ, Blachley T, Malatestinic WN, et al. Effectiveness of bDMARDs in ankylosing spondylitis patients by biologic use: experience from the CorEvitas PsA/SpA Registry. Curr Med Res Opin. 2024;40(2):315-23.
- Colombo D, Frassi M, Pagano Mariano G, et al. Real-world evidence of biologic treatments in psoriatic arthritis in Italy: results of the CHRONOS (EffeCtiveness of biologic treatments for psoriatic artHRitis in Italy: an ObservatioNal lOngitudinal Study of real-life clinical practice) an observational longitudinal study. BMC Rheumatol. 2022;6:57.
- Ramirez Huaranga MA, Calvo Pascual LA, Velasco Sanchez D, et al. Real-World Experience With Janus Kinase Inhibitors in Immune-Mediated Diseases: Clinical Experience of a University Hospital. Cureus. 2024;16(8):e67729.
- Wolfe F, Michaud K, Busch RE, et al. Polysymptomatic distress in patients with rheumatoid arthritis: understanding disproportionate response and its spectrum. Arthritis Care Res (Hoboken). 2014;66(10):1465-71.